

The reduction in infection and mortality rates of the 60-180mg intermediate ivermectin group
The latest Brazilian population-based study compared the <60mg irregular users and >180mg regular users vs. non-users of ivermectin. What about the 60-180mg group?

Several days ago, Dr. Lucy Kerr, Dr. Flavio Cadegiani and their colleagues published another excellent paper based on the data collected from the city-wide prophylaxis program in the Brazilian city of Itajaí showing massive reductions in hospitalization and mortality rates of more than 90%. They had detailed information for each citizen that participated in the program including data on the total amount of Ivermectin taken during the 6-month study period. Based on that, they identified, analyzed and compared three groups:
45,716 non-users
33,971 irregular users (total amount of less than 60 mg of Ivermectin)
8,325 regular users (total amount of more than 180 mg of Ivermectin)
In Figure 6, they summarized an overall view of the findings.
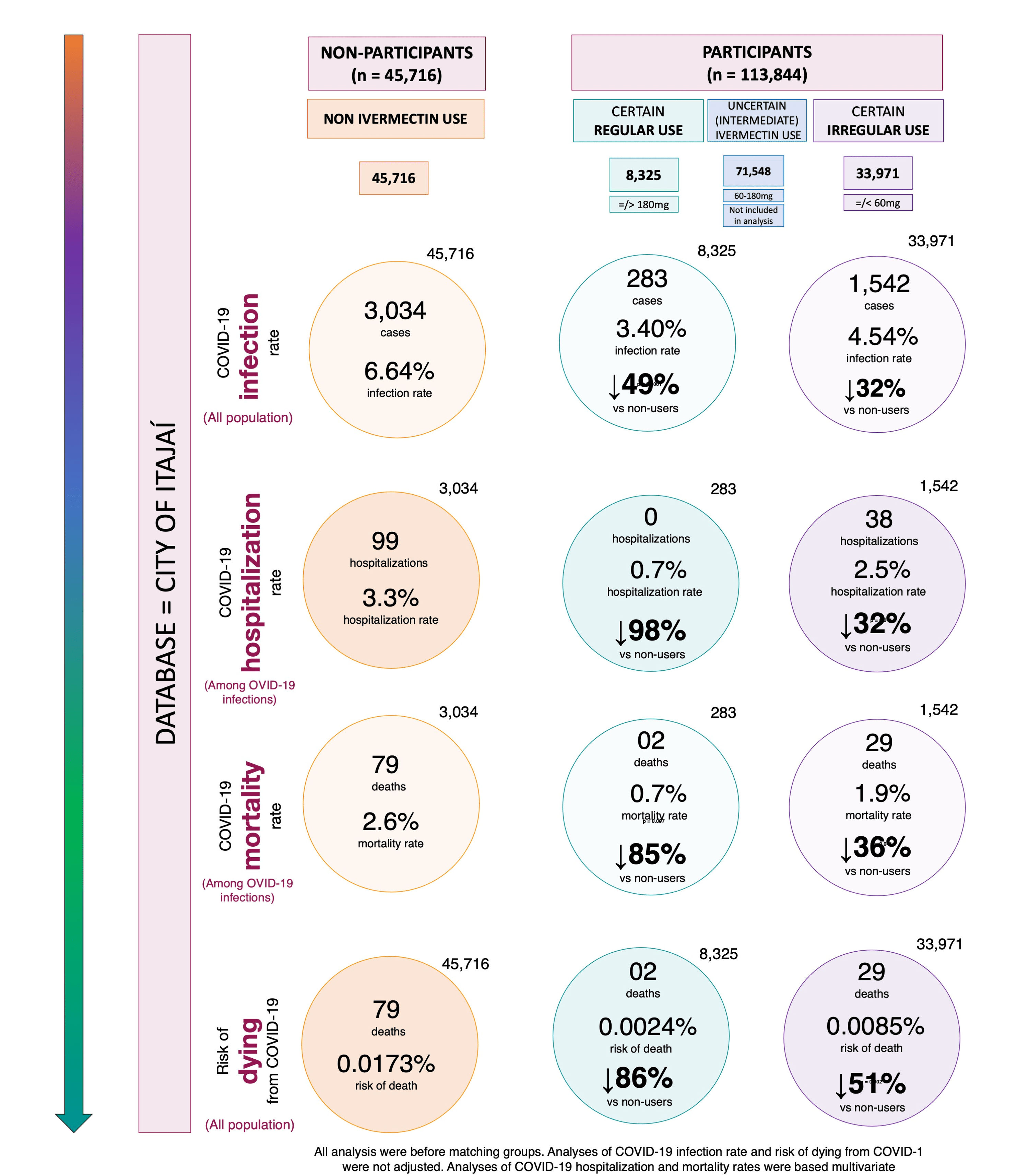
What about the 71,548 users which the authors called the “uncertain (intermediate) ivermectin use“ group? These people used more than 60 mg but less than 180 mg of Ivermectin. For them, we are unable to conduct a propensity score match (PSM) analysis. Furthermore, we are even unable to adjust the hospitalization and mortality relative risks using multivariate analysis. Simply, because we don’t have the data.
However, we can find out how well they fared against infection and risk of dying from COVID-19. Using data from both this one and the first paper by the same authors. Exactly as was done in the paper in Figure 6. So, we are going to insert a separate column in Figure 6 encompassing the numbers calculated for this group.
Here is the updated Figure 6. Please note that some percentages in the original paper were mistakenly calculated (not really a big deal, but need to be corrected in the paper) so those numbers were corrected (in red color).

Even though we could not calculate the multivariate-adjusted hospitalization and mortality rate reductions, the following conclusions can be drawn:
In general, as expected, the 60-180mg group fared better with respect to hospitalization and mortality rates than the <60mg group and worse than the >180mg group.
The crude infection rate reduction of the 60-180mg group is comparable to that of the >180mg group (about 50%, interesting!).
The risk of dying from COVID-19 within the 60-180mg group was reduced by 75% compared to non-users. Again, this is somewhat worse than the >180mg group (86%) and better than the <60mg group (51%).
Overall, this simple analysis reinforces the conclusion about the inverse causal relationship between the cumulative prophylactic Ivermectin dose and severe COVID-19 outcomes. The more regularly they took Ivermectin during the prophylaxis period, the less hospitalizations and deaths they had.