5 Years Later: The Most Comprehensive Analysis of COVID Treatments Research
Brief story of the unsung heroes of c19early.org who have created invaluable - but unfortunately - massively undervalued, and even ridiculed wealth of statistical analyses

You may have come across this website in the last 5 years: c19early.org. It first launched in June 2020, presenting statistical analyses of papers on COVID treatments. In the first months of the pandemic, fear and uncertainty reigned due to the virus that spread globally and mercilessly killed the most vulnerable. Officially, effective treatments did not exist, although the truth is different. As early as March 2020, there was a highly effective therapy, but that is another story. Lockdowns were in force on half the planet, people were not allowed to leave their homes, and when they had to go out, they wore masks both indoors and outdoors. Children were learning from home. Despite the impossible conditions for a normal life, there was great hope that vaccines and drugs would soon arrive allowing us to return to our pre-COVID lives.

A huge number of clinical trials of potential treatments were being conducted around the world, and the results were often published on pre-print servers, without prior peer-review. As they generated new analyses, the people at c19early.org also posted them on their Twitter account. But who are these people?
Their identities are still unknown even after 5 years, and they have described themselves from the beginning as “PhD researchers, scientists, people who hope to make a contribution, even if it is only very minor.” They further say “you can find our research in journals like Science and Nature. We have little interest in adding to our publication lists, being in the news, or being on TV (we have done these things before but feel there are more important things in life now).”
The first meta-analyses in December 2020
When multiple studies on the same treatment, for example vitamin D, were accumulated, the first meta-analyses were generated. A brief explanation for those who are not familiar with this term. Meta-analysis is a statistical method that combines results from multiple independent studies with control groups to obtain a more reliable and precise assessment of the studied effect. For example, if 10 studies examine the effectiveness of a drug for COVID, the meta-analysis will combine their results to determine whether the drug generally works and with what certainty.
So, back in December 2020, the first real-time meta-analyses of ivermectin, hydroxychloroquine and vitamin D appeared. All three indicated high effectiveness against COVID. This was the key historical moment when health regulatory agencies around the world officially approved, massively promoted and distributed these treatments to the entire world population. The virus was eradicated, and the pandemic suppressed by mid-2021. Unfortunately, only in some alternative history and universe.
Brutal censorship
Let's get back to the story. As soon as they presented the meta-analyses of these effective COVID treatments, suddenly and without any announcement or explanation, the Twitter account of this group was permanently banned. They were not on Twitter for two and a half years, and they were only reinstated in June 2023, after Elon Musk took over the social network. Those were times of harsh censorship on Facebook, Twitter, YouTube and other social media.
Their website could not be censored so they continued to work tirelessly and inform the whole world in real time about all effective and ineffective COVID treatments. Their 5-year work summarized in a few sentences:
“c19early analyzes over 5,800 studies for 169 treatments—over 17 million hours of research. US authorities believe only three high-profit early treatments reduce risk (remdesivir, paxlovid, molnupiravir). In reality, many treatments reduce risk, and 25 low-cost treatments have been approved across 163 countries. 0.6% of 9,000+ proposed treatments show reduced risk.”
Why should we believe these claims? They may be false.
Well, we shouldn’t. That’s the essence of the critical mind. Not to accept everything that is served by authorities at face value, but to observe and check skeptically. For example, listen to a TV interview with Anthony Fauci, the most famous American authority on infectious diseases (according to mainstream medicine, a kind of demigod) and then check Fauci’s claims. The same applies to the information presented on c19early.org. All their sources are public and verifiable. For the meta analyses, all data required to reproduce the analysis is contained in the appendix, with direct links to the original source papers.
What can we learn from their meta-analyses?
Nose and mouth treatment
Can you accept this simple realization, now after 5 years since the start of the pandemic and after such strong evidence? That, on first symptoms, treating the primary source of the initial infection (the nose, mouth and throat) dramatically reduces the risk of worsening the condition and the risk of transmitting the virus to other people. The most effective and efficient way to suppress the virus, to save yourself and others. Check out this summary chart of meta-analyses of povidone-iodine.

Immune Support
Vitamins A, C, D, and zinc reduce the risk of several adverse outcomes, similar to other viruses. The most important of these is vitamin D, for which a 2021 meta-analysis found that if your serum 25(OH)D3 concentration is above 50 ng/mL, your risk of dying from COVID is virtually ZERO. Knowing this, why haven’t health authorities in the US and EU recommended vitamin D supplementation?

Systemic Agents
Many systemic agents reduce the risk and may be needed when the infection progresses deeper than the upper respiratory tract.
At the top of this list is the prematurely “disqualified” hydroxychloroquine with strong evidence that it is effective for prophylaxis and early treatment. If it is used as a hospital treatment according to the FDA emergency use authorization in March 2020, then you will not see any benefit from it. Did they do it on purpose? Well, if you give toxically high doses to those hospitalized for COVID, it can be dangerous. That is exactly what they did in the large clinical trial in 2020 called RECOVERY conducted by a team at the University of Oxford. Was it on purpose?
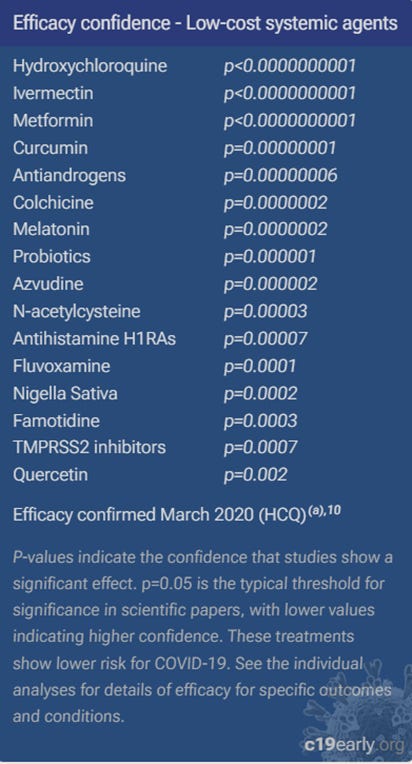
The “horse dewormer”
Do you also notice ivermectin, second on the list? The “horse dewormer”? Exactly the one that according to the US FDA, the WHO and almost all regulatory agencies in the world, is ineffective against COVID. Now, pay attention, the parameter p is the probability that the effectiveness of a given treatment is due to a random chance. So, according to the meta-analysis of ivermectin for COVID, the pooled effectiveness of ivermectin across all outcomes is 60% in 105 studies with a total of 220 thousand patients, it reduced mortality by almost 50% on average, and the p value is less than 1 in 10 billion. So, the chance that ivermectin is ineffective for COVID is less than 1 in 10 billion.
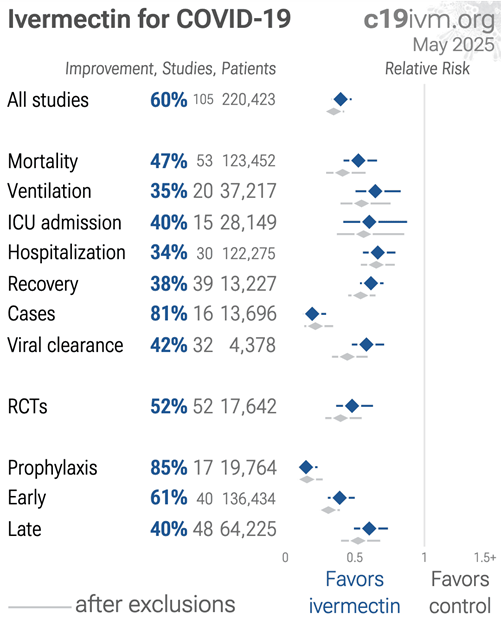
The flawed studies
There are several studies (e.g. PRINCIPLE, TOGETHER, ACTIV-6), in which, in addition to identifying numerous problems of a critical nature with the design and conduct of the studies, some of the authors are people with potentially serious conflicts of interest. These randomized clinical trials “found” that ivermectin is ineffective. But always keep in mind, this is exactly why a meta-analysis of all valid studies is done - to calculate the pooled effect. There are currently 105 valid studies, not 6 or 7. Even though these few expensive, large, but seriously flawed studies have seriously contaminated the meta-analyses for ivermectin, the average risk reduction across all 105 studies is 60% with a 95% confidence interval [52%-67%]. This is such a robust result that in a worst-case sensitivity analysis with exclusion, as many as 63 of the 105 studies must be excluded to avoid finding statistically significant efficacy.
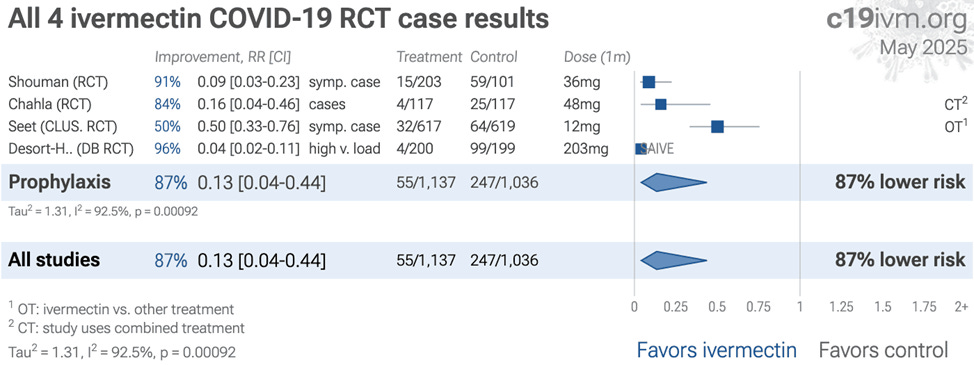
Ivermectin prophylaxis studies are completely ignored
It is striking that health regulatory agencies as well as the mainstream medical community have completely ignored ivermectin prophylaxis studies. In fact, they constitute the strongest evidence that ivermectin works because they show very high efficacy for preventing COVID infection, 81% according to a meta-analysis of 16 studies (with 14,000 subjects) and 87% according to a meta-analysis of randomized controlled trials (with about 2,200 subjects). Why are they ignored?

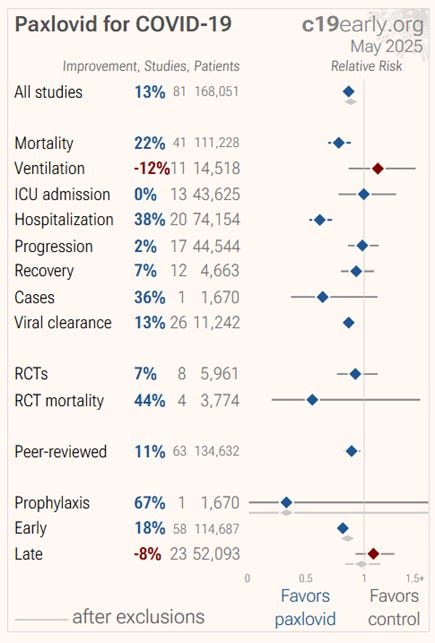
High-profit systemic agents
There are high-profit systemic agents that are also effective, but are less available and much more expensive. For example, paxlovid, Pfizer's early treatment drug, from 81 studies with a total of 168 thousand patients, has an aggregate efficacy of 13%, and reduced mortality by an average of 22% (statistically significant). Clearly, much less effective than ivermectin, but many governments around the world have signed contracts with Pfizer worth billions of dollars. On the other hand, for ivermectin, everyone parrots that it is ineffective. Because it is off-patent and cheap?
Acetaminophen
Acetaminophen, also known as paracetamol or tylenol, increases the risk of severe outcomes and mortality. I don't know if you remember, but during 2020 and a good part of 2021, Western health authorities, including the US and Australia, recommended that COVID patients stay home, take paracetamol, and when they turned blue due to hypoxia and saturation below 93%, go to the hospital. According to the meta-analysis of tylenol, essentially, health authorities (unintentionally or intentionally) recommended to citizens a therapy that brought them closer to death. Look at the meta-analyses of paracetamol. It increases the risk of mortality by 24%. Statistically significant result.

Remdesivir
Remdesivir was (and believe it or not, it still is!) part of the hospital protocol for treating COVID in the US. Look at the numbers in its meta-analyses. It does not reduce short-term hospital mortality (follow-up of up to 45 days). If patients are followed for a longer period of time after discharge from the hospital, from 2 to 3 months, mortality increases up to 20%. This is a result of the fact that remdesivir seriously damages the kidneys and liver. To make matters even more absurd, this agent is still recommended by the NIH in the hospital protocol for COVID. Insane but true.


Effectiveness vs. Cost
Based on meta-analyses of all treatments and their market prices, the folks at c19early.org created an interesting diagram in which the more effective the treatment is, the higher it is in the picture. Also, those in red are (very) expensive treatments. The following pattern is observed:
- The most effective treatments are the cheapest.
- The least effective treatments are the most expensive.
- Many of the expensive treatments are not only ineffective, but also increase risk.
It would be funny if it weren’t so sad.

The icing on the cake: a meta-analysis of meta-analyses
Finally, an extremely important, and at the same time, fun fact. The faithful followers of mainstream medicine, and thus indirectly of the big pharmaceutical industry, who understand something about statistics, have been parroting throughout the COVID pandemic that the vast majority of studies on cheap treatments such as ivermectin, hydroxychloroquine, vitamin D, melatonin, zinc and others are observational, i.e. non-randomized controlled studies, and therefore have a built-in defect and can only detect correlation (association), but not causation. In other words, they have no value in public health. For example, if ivermectin was given to one group of patients, and another group of patients refused or were unable to receive it, and if the ivermectin group had a significantly lower mortality rate, even if the results were adjusted for many baseline parameters, it could not be concluded that ivermectin was the one that reduced mortality because the patients in the groups were not randomly selected in advance (randomized). While this is potentially a valid argument, rejecting observational studies a priori is, to put it mildly, wrong. What is the contribution of c19early.org to this issue? They decided to test the hypothesis: do the pooled effects of randomized studies differ statistically significanly from the pooled effects of non-randomized studies? If there is a statistically significant difference between them, then, in general, it is most likely due to the unequal baseline characteristics of the treated and untreated groups in non-randomized studies.
Can you guess what their result was? I couldn’t believe it either when I looked at the so-called forest plot of the mega meta-analysis of 102 meta-analyses. The result in their own words:
“For the 102 treatments we cover, there is no difference in results between RCTs & observational studies, RR 1.00 [0.92-1.08].
For the subgroup of high-profit treatments, there is a non-significant trend towards greater efficacy in RCTs. This may be related to financial conflicts of interest.”
In simple terms, this result is interpreted as follows: observational, non-randomized controlled trials of COVID treatments were as valid as randomized trials in determining causal relationships between treatments and clinical outcomes.
End of story.

By the way, this is not the first meta-analysis of meta-analyses to compare randomized and non-randomized trials. In 2014, Engelmayer et al. published a Cochrane review/meta-analysis of 15 reviews that included 1583 meta-analyses for 228 different medical conditions with an average of 178 studies per paper. They concluded that:
“on average, there is little evidence for significant effect estimate differences between observational studies and RCTs”
So much for RCT puritanism.

Unsung Heroes
For 5 years, the unsung heroes of c19early.org have created a priceless, but unfortunately, massively undervalued, and even ridiculed wealth of statistical analyses of all possible clinical trials of COVID treatments, updated on a daily basis, which in the dark times of the pandemic served as a significant roadmap for thousands of doctors to identify the most effective, safest, and most affordable treatments for their patients who were desperately seeking relief from the vicious disease. Thanks to their selfless hard work, countless lives were spared from agonizing suffering and death. Unfortunately, the lucky ones were a tiny minority.
A great tribute. I was deeply impressed by their work back then as well. I learned so much from them. Wish them and you all the best!